



Poor quality of care is killing people. Conventional approaches to improve care have not been effective. To reverse this, Jhpiego is working with ministries of health in five countries in Africa through the Global Fund’s Quality Improvement and Leadership and Management project so that health workers have the skills to provide the right care to the right people at the right time.
In Nigeria, Jhpiego collaborates with the government from the national to the local level in Jigawa state, where we support 30 project facilities and organize peer-to-peer quality improvement meetings among facilities working on similar problems. We also focus on building the leadership and management capacity of government officials so that the Ministry of Health will be able to oversee, advocate for and scale up quality improvement approaches after the project ends.
Identifying overuse of antibiotics in malaria patients in Nigeria

As part of the peer-to-peer quality improvement process in Jigawa, in April 2022, our team reviewed malaria care data with health workers and local government area staff in each of the 30 facilities. January to March 2022 data showed that, on average, 98% of clients who had a positive test for malaria received first-line treatment. Of these clients, 55% also received antibiotics—a shockingly high number. Overall, the prevalence of severe bacterial co-infection among people with malaria is around 10%—and only clients with severe bacterial co-infection should receive an antibiotic.
Digging deeper into the data, we found significant variations in practice between the 30 facilities (Figure 1). Twelve health facilities prescribed antibiotics to 100% of people with a positive malaria test. Seven facilities did not prescribe antibiotics to any malaria clients, meaning that people who needed an antibiotic may not have received one. Both over- and under-prescription pose a challenge to the quality of care people receive.
Using variation in data to encourage reflection and change practices
Variations in practice indicate a problem—if facilities vary in their provision of care, then some facilities may be providing poor care. Used correctly, variations can be a source of learning and a powerful driver of behavior change. So, instead of using conventional training approaches—providing feedback on the consequences of over- or under-prescribing antibiotics—we organized meetings for health workers from different facilities in each of the three local government areas. Using peer-to-peer learning, we shared data from all the facilities and encouraged participants to reflect on their practice, compare it to others and learn from their peers.
Initially, the health workers justified their practices. But, as the discussions went on, they agreed that the amount of variation in the data could not be due to differences in clients. It must be a difference in the care they were providing. They decided to return to their facilities and determine what was driving their practices and address any problems they found.
Back at the facilities, Jhpiego and the Ministry of Health supported health workers to use a four-step group problem-solving approach (Box 1) to analyze their practices and improve care of people with malaria.
In the following months, during data reviews we saw that, overall, facilities were improving their use of antibiotics (Figure 2). In November, the average had dropped to 18%—well below the baseline average of 55%. All 12 of the facilities that had been prescribing antibiotics to 100% of clients reduced their use of antibiotics. Five of the seven that never prescribed antibiotics started identifying clients with bacterial infections and prescribing antibiotics.
Looking at the bigger picture
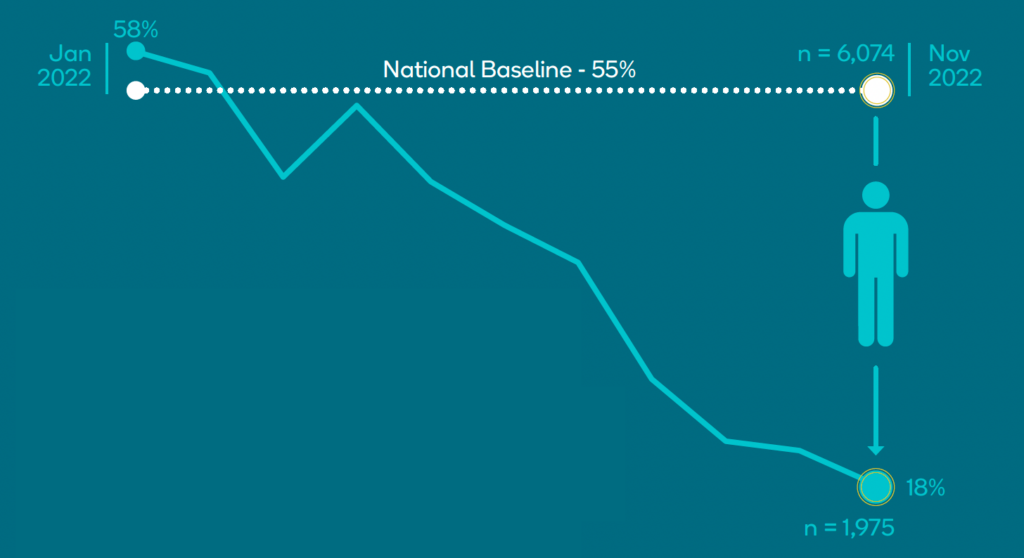
If prescriptions of antibiotics in November had been the same as the baseline, then 6,074 people would have received antibiotics compared to the 1,975 who did receive them. As a result of the peer-to-peer quality improvement work, 4,099 people who didn’t need treatment were not prescribed antibiotics. This saved the system $5,000 per month. It also reduced the risk of adverse events, work for pharmacists and pressure leading to antimicrobial resistance. It also reduced costs for clients—antibiotics cost about $1.20, the average daily income of most people in rural communities in Nigeria.
Nigeria has roughly 50 million cases of malaria each year. If management of malaria nationally is comparable to the January–March baseline, then roughly 25 million people are receiving antibiotics unnecessarily, at a cost of tens of millions of dollars per year. Increased use of group-based problem-solving and peer-to-peer support to highlight variations in practice could help reduce unnecessary antibiotic use and help ensure that those who need treatment will receive it—the right people get the right care at the right time
This evidence-based approach to thoughtfully consider the true problem, identify solutions, test changes and measure success led to direct improvements in quality of care for clients and significant cost savings for the health system. It is exciting to see the use of simple, yet evidence-based approaches improving outcomes for those we serve.”
Julia Bluestone, Jhpiego’s Health Workforce Team Lead
Yemisi Ogundare is Jhpiego’s Project Lead for the Global Fund Quality Improvement and Leadership and Management project in Nigeria. Nigel Livesley is Jhpiego’s Technical Director for the Global Fund Quality Improvement and Leadership and Management project.